Step 2 CS Blue Sheet Chronic Cough Case:
Here are the blue sheet, physical exam, diagnostic studies, and differential diagnosis needed for a chronic cough case in the USMLE Step 2 CS exam:
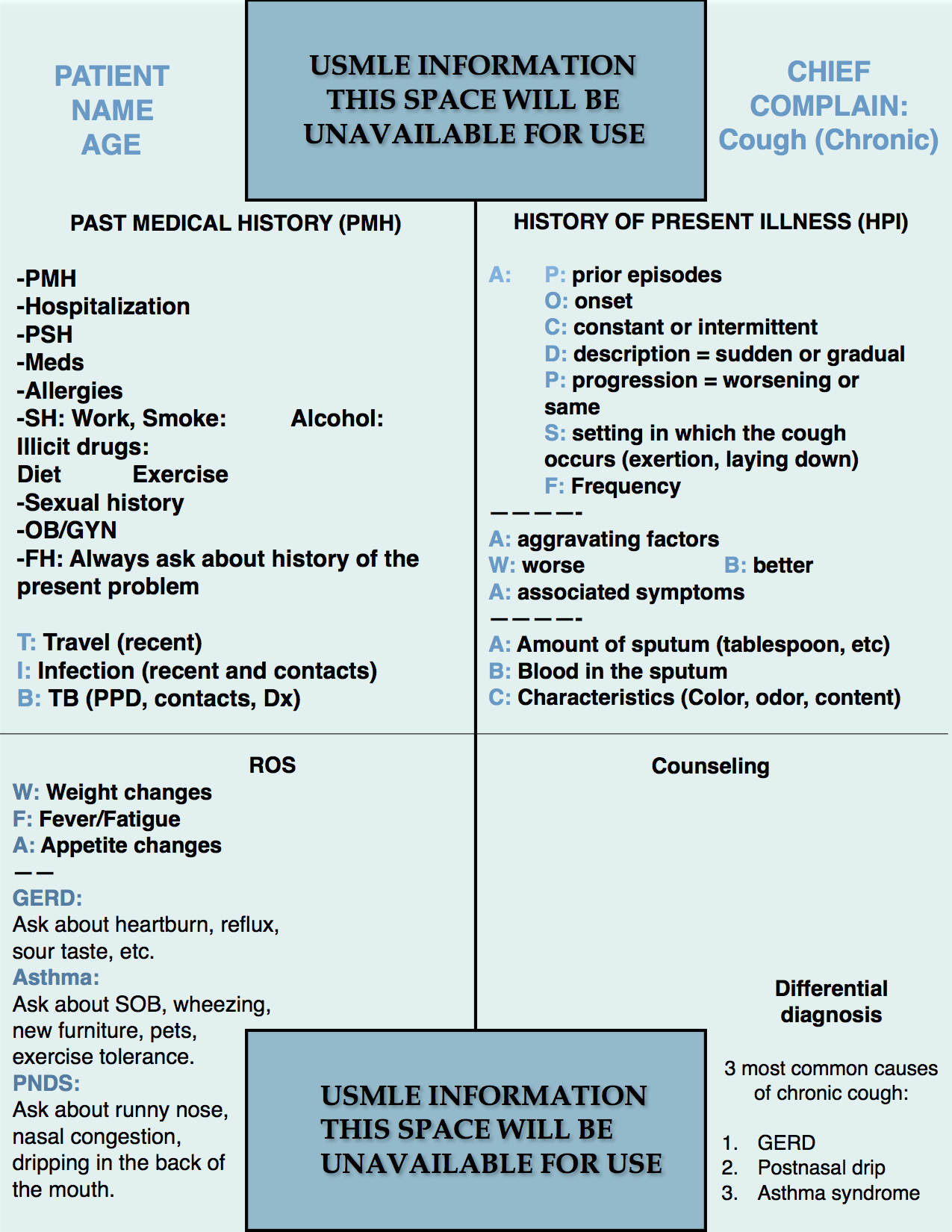
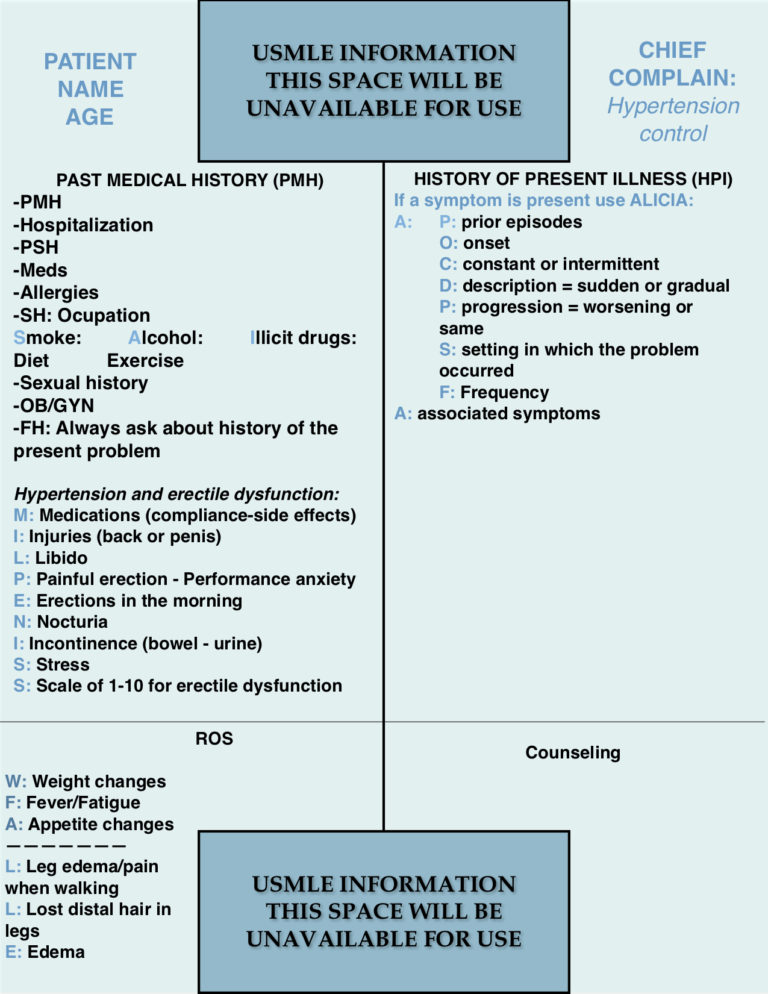
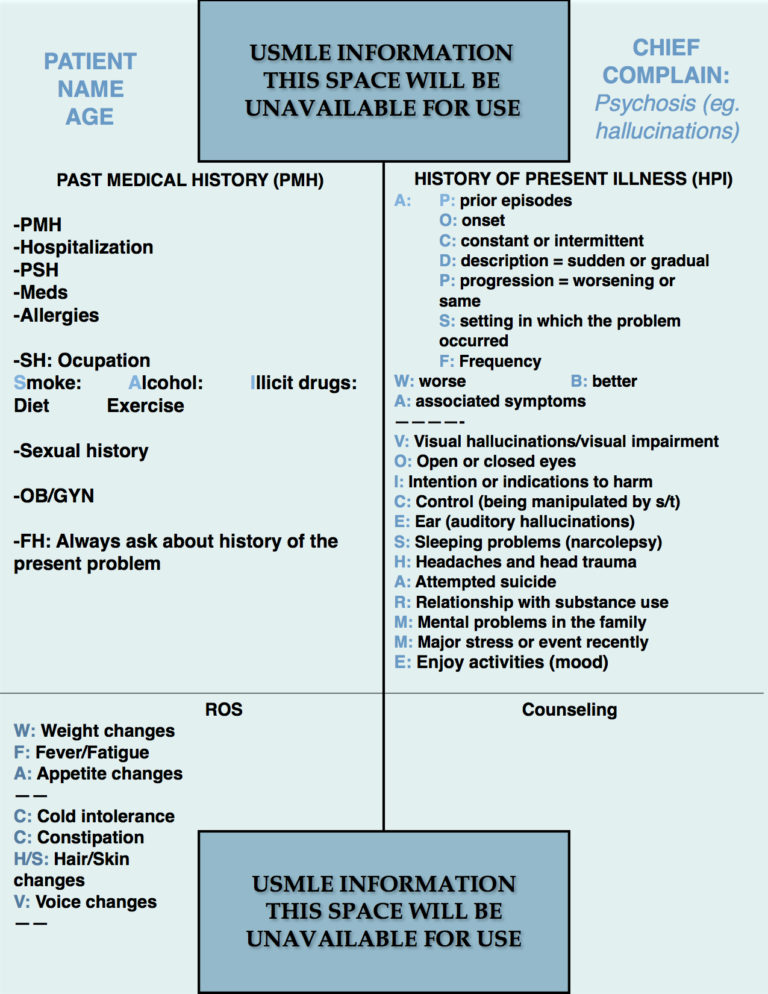
For a chronic cough case, it is important to add a few parts to our blue sheet structure:
1. In the past medical history, add “TIB” that stand for recent travel, infections and TB history and/or exposure. This allows one to recognize risk factors such as a patient traveling to an area known to have increased risk of acquiring a lung infection. For TB patients is important to recognize the risk factors such as recent immigration from an underdeveloped country, recent imprisonment, or contact with a person known to have tuberculosis.
2. The “ABC” for sputum: Write those three letters in your blue sheet to remember asking about sputum accompanying the cough. The letters ABC allow one to ask about the amount of sputum (tablespoon, teaspoon, cup, etc), blood in the sputum, and its characteristics such as color, odor, thickness.
3. The three most common causes of a chronic cough in up to 90 % of the cases are GERD, postnasal drip syndrome or PNDS, and bronchial asthma. Therefore, it is very important to ask questions about them to identify a possible case or to rule it out.
PHYSICAL EXAMINATION
Vital signs:
Look for fever and tachycardia (secondary to fever). Some authors describe the combination of fever and bradycardia for certain pulmonary infections such as typhoid fever, Legionnaire’s disease, and pneumonia caused by Chlamydia sp. However, relative bradycardia as a clinical sign has no predictive value for obtaining a tentative diagnosis and one can use it as a sign that will add to others in making a diagnosis.
Relative bradycardia in infectious diseases – https://www.ncbi.nlm.nih.gov/pubmed/8945708.
1. HEENT:
Inspection of the nose, mouth, and throat for signs of infection. Thrush may be present and it can represent a sign of HIV infection or others.
Palpation of the face and sinuses looking for tenderness when there is suspicion of sinusitis.
Neck: Look for lymphadenopathy, masses, assessment of the thyroid gland for masses or enlargement, and jugular venous distention (for congestive heart failure for example.)
2. Lungs:
Inspection
Palpation
Percussion
Auscultation. Beware of what the patient does since they can move the thorax without performing inspiration and that can indicate a decreased air entry in the area of auscultation.
3. Heart:
Palpation of the point of maximal impulse (PMI).
Auscultation.
3. Extremities:
Inspection: look for edema, cyanosis and/or clubbing.
6. Skin:
Inspect for generalized cyanosis or pallor.
POSSIBLE DIAGNOSTIC STUDIES:
- Pulse oxymetry.
- CBC with differential.
- ESR, CRP.
- Sputum analysis: gram, acid-fast stain, culture.
- Chest X-ray.
- Pulmonary function tests PFT or peak expiratory flow rate PEFR.
- ABG or arterial blood gases.
- HIV, VDRL.
- Urine legionella antigen.
- Serum mycoplasma PCR.
- Cold agglutinins for mycoplasma infection
- ECG, echocardiogram.
- Bronchoscopy with bronchoalveolar lavage.
The tests that can be asked here are broad and depend on the patient’s presentation. It is not necessary to order all of them in every patient. In fact, the workup should be as specific as possible to practice a cost-effective and safe assessment of the patients.
DIFFERENTIAL DIAGNOSIS:
- GERD.
- PNDS.
- Bronchial Asthma.
- Congestive heart failure.
- COPD.
- Chronic bronchitis.
- Upper respiratory infection associated cough.
- Sinusitis.
- Tuberculosis.
- ACE inhibitor-induced cough.
- Pulmonary embolism (when chronic, although it is usually acute in the presentation).
We hope that this post can help you better understand how to handle a chronic cough case in your exam. Please, feel free to contact us should you have any comment or question by using the comments section below. Good luck with your studies.

- Aortic Stenosis Severity Classification - 09/22/2020
- Carboplatin (Paraplatin) - 04/07/2019
- How to test for Vitamin D deficiency? - 09/29/2018