Objectives: Learn how to address a patient in the Step 2 CS exam, developing a standard way of approaching patients efficiently by using a structured plan for the clinical history, physical exam, closure, and patient note. Use mnemonics to help to guide the examinee during the patient encounter and patient note.
Step 2 CS Patient Encounter – Medical History to Closure (With Mnemonics)

The patient encounter is composed of four major parts: the clinical history taking, physical exam, closure and patient note. It starts with the doorway information and finishes after one has finished typing the patient’s note. The actual encounter with the patient at the examination room determines the final scores of the CIS (Communication and Interpersonal Skills) and the SEP (Spoken English Proficiency) parts of the Step 2 Cs exam. The physical examination and patient note are the two pillars of the ICE (Integrated Clinical Encounter) section. Therefore, learning to approach the patient encounter in a standardized and efficient way is crucial for passing the exam.
1. ClINICAL HISTORY TAKING
The best aid to use during the exam is the blue sheet of paper that the examination center will provide to the examinees. Information about how to use this blue sheet as the best helper tool during the exam will be described continuously throughout this publication. Remember to make a transition statement when changing from one part to another. For example, when switching from the past medical history to the history of present illness, one might say, I would like to ask you about your current problem now, please?
DOORWAY INFORMATION
Before a case starts in the USMLE Step 2 CS exam, basic information about the patient will be described such as the name, age, gender, chief complaint, vital signs (if abnormal), indications for the case, etc. Nevertheless, the most vital use one can give to the doorway information is the preparation for the case that is going to be done. There are two important aspects to keep in mind:
- Making a mental differential diagnosis for the chief complaint that the patient holds. The more focused on the patient the better. For example, a patient with chest pain can have more probability of having a myocardial infarction if his age is >50 years old versus a younger patient.
- Writing down important information on the blue sheet that you may forget due to nervousness or lack of time to think during the encounter or patient note. What you can write involves mostly the differential diagnosis and mnemonics.
The time taken at the doorway should be the required for the applicant to be prepared to approach the case with confidence and clarity of mind. The standard time is 10-20 seconds (First Aid). However, in practice, it can take around 45 seconds to a minute to be ready to go in after writing down all one may need. The time is variable depending on the examinee preference, thus it is crucial to practice and set the most convenient time for each individual.
PATIENT GREETING
The classic rules of greeting should be used:
- Knock the door before going into the room.
- Verify the patient’s identity by asking, “Good morning, Mr. Jones?”
- Keep eye contact as much as possible.
- Introduce yourself, “Hi, I am Dr. X, nice to meet you.”
- Shake hands firmly but gently. Do it with confidence and keep eye contact (handshake is important in the United States). [1]
- Drape the patient (most patients seen in the exam will be already draped).
THE CLINICAL HISTORY
There are two ways of taking a clinical history (both of which generally start by asking the patient something like, what brings you in today?:
- Starting with the history of present illness (HPI): After asking what can I do for you today? and getting a reply such as, “I feel dizzy,” one can continue asking about the dizziness. Hence, finishing the history of present illness first and then moving on to the past medical history.
- Starting with the past medical history (PMH): After asking, how can I help you today? and getting a response like, “I have a headache,” one can transition into the past medical history saying, “I am sorry about that. Please, let me ask you about your background to better understand your current problem, all right? After finishing the PMH, one can continue with the HPI.
Which one is better is up to the examinee. There is an advantage of asking first about the past medical history, which is that you will be more oriented as to what is the most feasible cause of the chief complaint. A hypertensive and diabetic patient experiencing chest pain suggests more a cardiovascular cause comparing to a patient with chest pain and unknown history. Both options are fine as long as one does not neglect any of the important parts of the clinical history. Practice both of them and use the one that fully suits your needs.
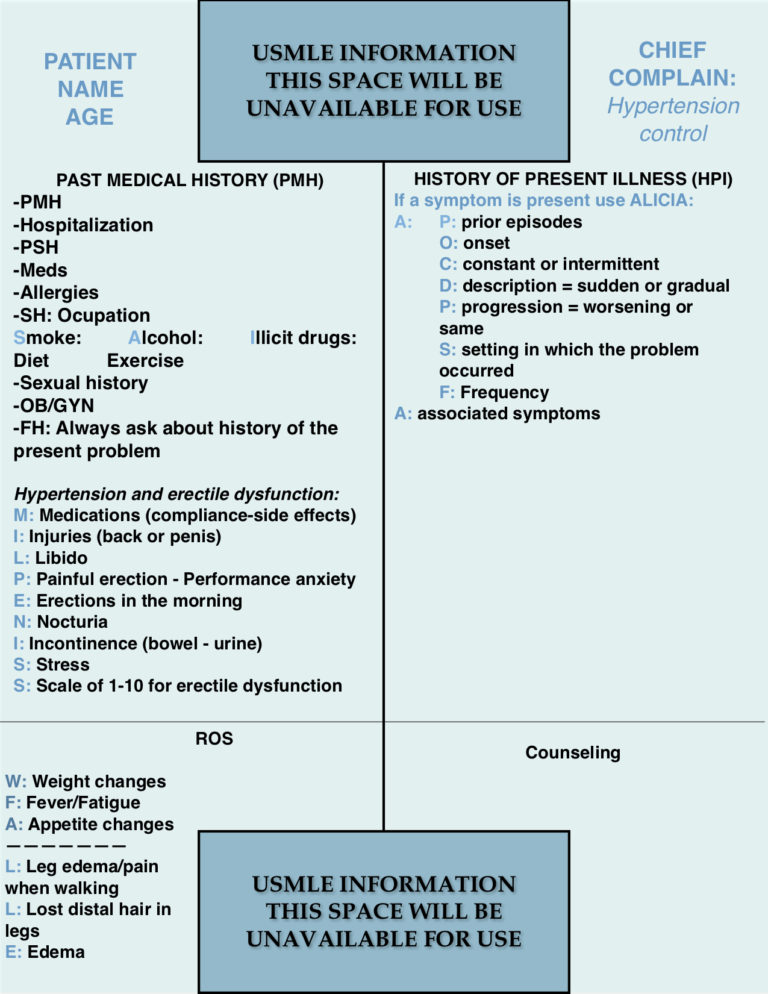
PAST MEDICAL HISTORY
There is a structure that one can use to ask about the PMH, which is:
- Past medical history: Ask about the past medical history, for example, “Have you ever been diagnosed with any medical condition?” Ask all about the disease like when it was diagnosed, for how long it has been present, treatments, and so on.
- Hospitalizations: Have you ever been hospitalized before?
- Past surgical history: Have you ever had any surgery in the past?
- Medications: Are you taking any medications? Ask about prescribed and over the counter drugs.
- Allergies: Do you have any allergy? Ask about allergies to medications, environmental elements, and the reaction originated from the exposure (eg. rash).
- Social history: Occupation, diet, exercise. Also, ask about the important 3 bad habits: “SAI” smoking, alcohol and illicit drugs consumption. It is important to ask for when it started, how long it has been going on, the quantity used and the intention or attempts to quit the substance use. One can advise quickly about the advantage of quitting right away at this point, releasing some of the tasks needed to be done at the closure.
- Sexual history: Ask about sexual behavior, partners, and safety taken.
- OB/GYN: Ask about obstetric history (gestations, parturitions, abortions, cesareans, etc.) G1P1A0C0. Menstrual cycle, last menstrual period and anything else that you might consider important for the case.
- Family history: Always ask about the history of the present problem. For example, if a patient is experiencing psychotic symptoms, asking about family history is important to identify a primary psychiatric disorder. Ask about direct family members (parents, brothers, and offspring).
The sexual and OB/GYN history are not always necessary to take. Thus it is at the examinee’s discretion if it is necessary to take them. In case of doubt, it is better to do it superficially unless otherwise required.
It is NOT necessary to use mnemonics for the past medical history. The reason is that the PMH is done almost in the same way for all cases and if practiced frequently enough, one will probably memorize it with ease. However, a mnemonic such as PAM HUGS FOSS can be used.
HISTORY OF PRESENT ILLNESS (HPI)
One can start with the chief complaint and then continue asking in detail what is relevant. Do not forget to show compassion when a patient states experiencing a symptom such as pain. A simple phrase like, “I am sorry that you are experiencing this pain” or “That must be difficult for you” helps to build rapport with the patients.
Using a mnemonic is recommended for the history of present illness. There are several mnemonics that may be used for the HPI. “ALICIA,” a mnemonic frequently used in South America can be of useful guidance. CC LIQUORA or another similar mnemonic may also be used. There is no difference regarding which mnemonic one utilizes. Always ask if that is the first time that the chief complaint is present.
- A: Antiquity or age. Refers to the antiquity or age of the current problem. This letter has its own mnemonic P-OCDPSF
- P: Prior events.
- O: Onset. When did it start?
- C: Constant or intermittent. Is the problem always present or does it comes and goes?
- D: Duration. If constant ask when it started. If intermittent (episodic), ask when did the episodes started and how long they last.
- P: Progression. Is the current problem worsening, the same, or getting better.
- S: Setting in which it occurs. What were you doing when the pain started?
- F: Frequency. How many times a day, week, or month does it occur?
- L: Localization of the symptom such as pain.
- I: It travels through the body or not? Radiation of the pain.
- C: Characteristic of the pain. Is the pain sharp or dull?
- I: Intensity. On a scale of 1 to 10, how would you rate your pain/symptom?
- A: Aggravating and alleviating factors (two A’s). What makes it better? What makes it worse?
- A: Associated symptoms with it.
REVIEW OF SYSTEMS (ROS):
The review of systems should be focused on the current problem and special case needs. For example, a patient presenting with fatigue needs to be asked about the presence of constitutional symptoms. Therefore, learning a few short mnemonics for such cases may help:
To screen for constitutional symptoms, infections, and other systemic disorders:
WFA mnemonic
- W: Weight loss or gain (unintentional).
- F: Fever or chills.
- A: Appetite changes such as anorexia.
To screen for thyroid disorders:
C-C-H/S mnemonic
- C: Constipation or diarrhea.
- C: Cold or heat intolerance.
- H/S: Hair and/or skin changes such as dry skin or alopecia.
To screen for neuropathic damage and neurologic disorders such as stroke
T-N-W mnemonic
- T: Tingling (sensory nerve disorder).
- N: Numbness (sensory nerve disorder).
- W: Weakness (motor abnormalities).
Tingling, numbness, and weakness should be asked together if possible. They screen for neuropathy and motor abnormalities.
There are other very important mnemonics that are useful in specific cases. They are described in every chief complaint described in the Step 2 CS publications on this website. Please, visit the following link for more information.
PHYSICAL EXAM
The physical exam should be focused and simple. It is not necessary to perform a complete physical exam in all patients during the Step 2 CS exam nor there is time enough for doing so. There are some general considerations to follow:
- Make a transition statement when planning to start the physical exam. For example, “Thank you for answering my questions. I have finished the interrogation and now I would like to examine you if you don’t mind?
- Wash your hands or wear globes (faster choice and totally acceptable).
- Be gentle. Patients will tell you if they have pain even with the slightest touch.
- Do not perform breast, genital, rectal exams or corneal reflex. Follow the USMLE indications.
- Say thank you when a patient does something you asked her/him to do.
- Be attentive to the simulated symptoms such as thoracic movement without actual movement of air into the lungs pointing to decreased breath sounds in the area of auscultation.
Since the physical exam should be focused, it is recommended to review the required physical exam recommended for each chief complaint as described in the Step 2 CS blue sheet cases section of this website.
CLOSURE
The final step in the examination room should be the closure in which we give a clear diagnostic impression to the patient, recommend what can be done such as workup and medical instructions regarding diet, smoking cessation, avoidance of alcohol, etc. The closure should be simple and in plain English depending on the patient’s level of education. Do not forget to ask, “Do you have any question for me?”
One does not need to provide a definitive diagnosis during the closure – that usually is not feasible to make. Therefore, give your opinion to your patient about all the possible causes from the most probable to the least, outlining what is your recommendation to reach a final diagnosis is and clarifying any question or concern the patient may have regarding his health.
This finishes the clinical history taking section of the USMLE Step 2 CS exam. The key for the USMLE Step 2 CS exam is to practice over and over the cases, ideally with a real person (study partner or anyone else).
Please, if you have any comment, question, or suggestion, do not hesitate to write it down in the comments section below. Good luck.
References:

- Aortic Stenosis Severity Classification - 09/22/2020
- Carboplatin (Paraplatin) - 04/07/2019
- How to test for Vitamin D deficiency? - 09/29/2018




Can we say to patient to after physical exam that ” I would prescribe you some pain medicines”
Hi. Yes, counseling does not need to be very specific. You can say: “I think you have a throat infection and I can offer you some pain medications for that.” Do not need to specify dosing or side effects. If there is time that would be ideal but usually that is not the case. The most important thing is to give the patient an overall impression of what is going on and the plan to address that problem. I hope this helps