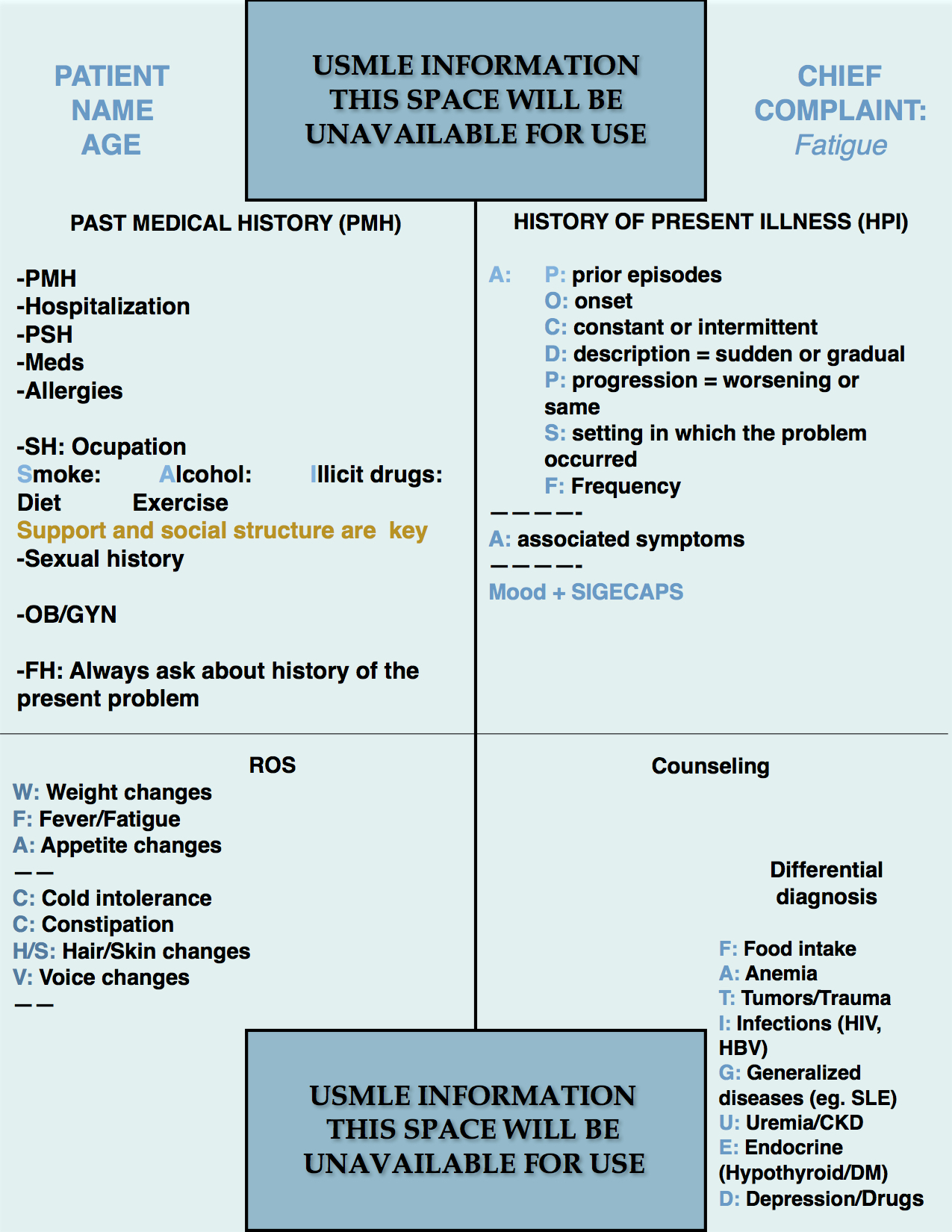
Step 2 CS Blue Sheet Fatigue Case:
Fatigue is one of the most common presenting symptoms in medicine and the USMLE exams. However, it is a non-specific clinical symptom and thus it needs an effective clinical history for narrowing down the possible differential diagnosis. Let us review the suggested blue sheet, physical exam, diagnostic studies, and differential diagnosis needed to be done for addressing fatigue in USMLE Step 2 CS exam:
As mentioned before, fatigue is a non-specific symptom that can be related to several conditions. Therefore, it is better to sum it to the other presenting symptoms that a patient may have for formulating a differential diagnosis.
IMPORTANT ASPECTS OF THE PAST MEDICAL HISTORY:
The PMH in a case of fatigue is similar to most cases but needs special attention when analyzing the social background. Asking about family structure, family and social support, home companions, caregivers, work situation, problems at home or work, and their mood is essential particularly in elderly people.
In younger people, risk factors such as risky sexual behavior (lack of barrier protection, multiple partners, etc) are also important since HIV, Hepatitis virus, and other infections can cause fatigue only.
IMPORTANT ASPECTS OF THE HISTORY OF PRESENT ILLNESS:
Again, if not done during the social history interrogation, asking about mood is very important. When the patient describes his or her mood as low, the mnemonic “SIGECAPS” helps to screen for depression:
S: Sleep problems.
I: Lack of interest.
G: Guiltiness.
E: Energy level decreased.
C: Concentration diminished.
A: Appetite changes.
P: Psychomotor retardation.
S: Suicidality (ideation, intention, plan).
PHYSICAL EXAMINATION:
1. HEENT/Neck:
- Eyes: look for conjunctival paleness (anemia), jaundice (liver disorders).
- Mouth and throat: look for lesions such as thrush (candida in HIV positive patients), ulcers in SLE.
- Neck: Perform thyroid exam, lymph node exam (Generalized LAD is seen in infections such as in HIV, infectious mononucleosis, and others.
2. Lungs:
- Auscultation only unless more is required (eg. patient refers a cough).
3. Cardiovascular:
- Auscultation of the heart.
4. Abdomen:
- Inspection: Look for vascular signs like caput medusae, telangiectasias (cirrhosis), scratch marks (cholestasis).
- Auscultation.
- Palpation: Screen for hepatosplenomegaly (seen in several infectious conditions).
- Percussion.
5. Skin:
- Look for changes in skin such as rashes, paleness, and jaundice.
6. Extremities:
- Inspection.
7. Neurologic:
- DTR’s for thyroid disease
WORKUP:
- Rectal exam.
- CBC.
- Stool FOBT.
- Fecal fat studies.
- Glucose, HbA1C.
- Liver function tests (LFT’s).
- Amylase, lipase.
- TSH, T4.
- ESR.
- HIV serology, hepatitis viral serology, VDRL.
- PPD, Chest X-ray (CXR), sputum analysis (Tuberculosis).
- Ultrasound of the abdomen.
- CT scan of the chest and/or abdomen.
DIFFERENTIAL DIAGNOSIS:
Use the mnemonic “FATIGUED” to remember the most important differential diagnosis to consider:
- F: Food intake (neglect in elderly patients or lack of support).
- A: Anemia.
- T: Tumors/Trauma/Tuberculosis. Malignancy is an important differential diagnosis in middle-aged and elderly patients.
- I: Infections (HIV, HBV).
- G: Generalized diseases (eg. SLE).
- U: Uremia/CKD.
- E: Endocrine (Hypothyroid/DM).
- D: Depression/Drugs of abuse.
We hope that this post can help you better understand how to handle a case of fatigue in your exam. Please, feel free to contact us should you have any comment or question by using the comments section below. Good luck with your studies.

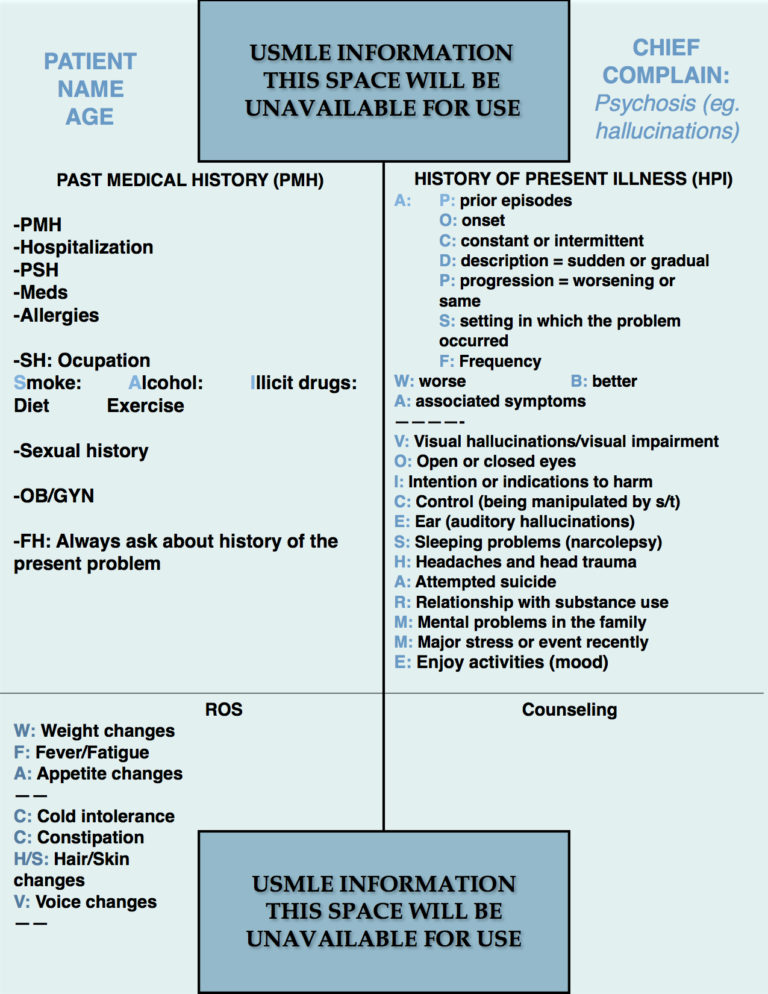
- Step 2 CS Blue Sheet Psychosis - 03/23/2018
- Step 2 CS Blue Sheet Memory Loss/Forgetfulness - 03/23/2018
- Step 2 CS Blue Sheet Shortness of Breath - 03/13/2018




Excellent publication. Thank you.